The 2026 MAT Compliance Playbook: Verifying Adherence in the Fentanyl Era

Medication-Assisted Treatment (MAT) is a cornerstone of modern opioid use disorder (OUD) management. The data is clear: methadone can reduce overdose mortality by 59%, and buprenorphine by 38%, according to the 2026 MAT Toolkit. But these life-saving outcomes depend entirely on patient adherence. In an era of increasing fentanyl prevalence and sophisticated diversion tactics, a simple positive or negative drug test result is no longer enough to ensure patient safety and program integrity.
Effective MAT monitoring has shifted from punitive testing to therapeutic monitoring. The central question for clinicians is no longer just “Is the drug present?” but “Is the patient taking their medication as prescribed?” Answering this requires a deeper understanding of drug metabolism and the specific markers that verify therapeutic use versus specimen manipulation. This guide provides a clinical framework for interpreting MAT drug tests to improve patient outcomes and maintain program compliance.
The New Compliance Paradigm: Moving Beyond Basic Screening
Traditional drug tests often look only for the parent drug, a method that can be easily defeated by “pill dipping” or “spiking,” where a patient adds a small amount of their prescribed medication directly to their urine sample. This produces a positive result while the patient may be diverting the bulk of their medication.
True therapeutic monitoring focuses on metabolites, the unique substances the body produces after processing a drug. The presence, absence, and ratio of these metabolites provide a clear, actionable story about a patient’s adherence.
Understanding these “truth markers” is the first step toward building a robust monitoring protocol. Each of the three primary MAT medications has a distinct metabolic signature that clinicians must be able to recognize.
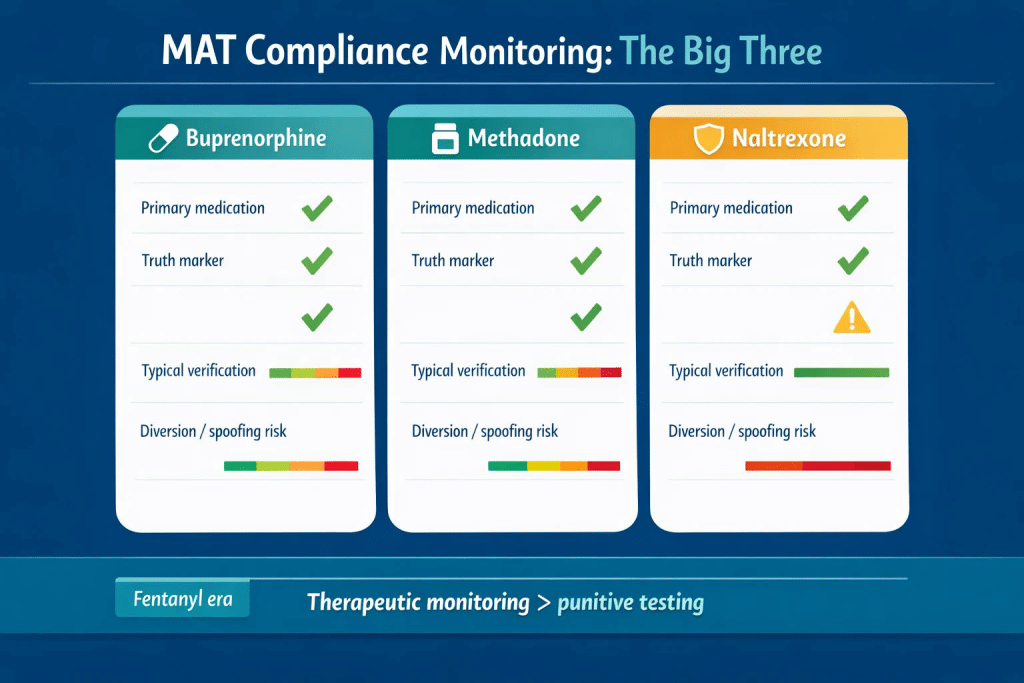
The Three Pillars of MAT: Key Metabolites for Verification
While buprenorphine, methadone, and naltrexone are all effective OUD treatments, they require different monitoring strategies. Focusing on the correct metabolite is crucial for distinguishing genuine compliance from potential diversion.
Buprenorphine: Decoding the Norbuprenorphine-to-Buprenorphine (N/B) Ratio
For patients prescribed buprenorphine (e.g., Suboxone), the most important substance to measure is not buprenorphine itself, but its primary metabolite: norbuprenorphine. When a patient takes buprenorphine as prescribed, their body metabolizes it, producing norbuprenorphine which is then excreted in the urine.
The ratio of norbuprenorphine to the parent drug (the N/B ratio) is the gold standard for verifying adherence. Research from Labcorp, based on over 100,000 results, provides clear clinical thresholds for interpretation:
- N/B Ratio > 0.3: This is the expected finding for a compliant patient. In fact, studies show that 95% of adherent patients have a ratio above 0.3, with most falling above 1.0. This indicates the body has properly metabolized the medication over time.
- N/B Ratio < 0.3: This is an atypical result that warrants clinical review. It could suggest a very recent dose, potential drug-drug interactions affecting metabolism, or inconsistent use. It is a signal to open a conversation with the patient, not an immediate conclusion of non-compliance.
- N/B Ratio < 0.02: This ratio is a definitive indicator of “spiking” or “pill dipping.” A finding this low is physiologically implausible and strongly suggests the parent drug was added directly to the urine sample. Data published in JAMA Psychiatry confirms this threshold as a reliable marker for specimen adulteration.

By analyzing the N/B ratio, clinicians can confidently distinguish between therapeutic use and attempts to deceive the test.
Methadone and Naltrexone: Identifying Their Unique Truth Markers
Similar principles apply to other MAT medications, each with its own key metabolite.
- For Methadone: The crucial metabolite is EDDP (2-ethylidene-1,5-dimethyl-3,3-diphenylpyrrolidine). A urine sample that is positive for methadone but negative for EDDP is highly suspicious for spiking, as EDDP is only produced through metabolism.
- For Naltrexone: The primary metabolite to look for is 6-beta-naltrexol. Its presence confirms that the patient has ingested and metabolized naltrexone. Verifying adherence is particularly important for naltrexone, as it is an opioid antagonist, and a patient who stops taking it is at high risk of overdose if they relapse.
Building an Effective Monitoring Workflow
A successful MAT monitoring program balances the need for immediate results with the demand for forensic accuracy. This often involves a two-step process that combines rapid point-of-care screening with confirmatory laboratory testing when needed.
- Point-of-Care (POC) Screening: The first line of defense is a rapid screening test performed on-site. Using reliable, CLIA-waived multi-panel drug test cups provides immediate, preliminary results. This allows clinicians to assess baseline adherence and detect unexpected substances during the patient’s visit. A high-quality 12 panel drug test cup can screen for MAT drugs alongside common drugs of abuse like fentanyl, providing a comprehensive initial picture.
- Confirmatory Testing (LC-MS/MS): When a POC test yields an unexpected or atypical result (e.g., a positive buprenorphine screen that raises suspicion of spiking), the sample should be sent to a laboratory for definitive analysis using Liquid Chromatography with Tandem Mass Spectrometry (LC-MS/MS). This is the only method that can accurately quantify drug and metabolite levels to calculate ratios like the N/B ratio.

This tiered approach is both clinically effective and cost-efficient. It allows programs to use affordable, rapid screening for the majority of encounters and reserve more expensive laboratory analysis for situations that require deeper investigation.
Managing the Atypical Result: A Guide to Clinical Conversations
An unexpected test result is a clinical opportunity, not a punitive event. How a clinician addresses a result suspicious for diversion can either strengthen or destroy the therapeutic alliance. The goal is to gather more information, express concern for the patient’s safety, and adjust the treatment plan accordingly.
When faced with an atypical result, such as a low N/B ratio, consider this structured approach:
Step 1: Review Clinical Context. Before speaking with the patient, rule out other possibilities. Could a new medication be interfering with metabolism? Is there any evidence of urine dilution (e.g., low creatinine levels)?
Step 2: Use a Non-Accusatory Script. Open the conversation with curiosity and concern, not accusation.
- Instead of: “Your test shows you’re not taking your medication.”
- Try: “I’m looking at your test results, and they’re a bit unusual. It looks like the medication isn’t processing in your system the way we’d expect. Can you tell me how you’ve been taking your Suboxone this past week?”
This invites dialogue and helps you understand the patient’s perspective.
Step 3: Escalate Care, Not Punishment. The response should be therapeutic. This may involve increasing the frequency of visits, exploring observed dosing, or referring the patient to a higher level of care if they are struggling.

The Final Word on MAT Monitoring
In 2026, MAT compliance is about clinical data, not just detection. By focusing on key metabolites and understanding how to interpret them, you can build a monitoring program that truly supports patient recovery. It ensures that life-saving medications are being used effectively while protecting the integrity of your program.
At 12 Panel Now, we are committed to providing affordable and reliable tools that empower clinics to implement these advanced monitoring strategies. By combining high-quality POC screening with an informed clinical approach, you can confidently navigate the complexities of MAT adherence and guide your patients toward lasting recovery.