A provider’s guide to opioid stewardship and patient adherence

Clinical data suggests up to 50% of chronic pain patients may have at least one “unexpected” urine drug test result during their treatment. This single statistic from the American Society of Addiction Medicine highlights the central challenge in modern pain management: balancing effective care with responsible opioid stewardship. An unexpected result is often seen as a sign of non-adherence or diversion, but the reality is far more complex. For clinic managers and providers, navigating these results is crucial for maintaining regulatory compliance, ensuring patient safety, and preserving the provider-patient relationship.
A successful drug testing protocol isn’t about catching patients; it’s about protecting them. It confirms they are taking their prescribed medication, identifies the presence of dangerous non-prescribed substances, and provides the objective data needed to make sound clinical decisions. This guide will walk you through the science of test interpretation, the nuances of patient communication, and how to build a testing protocol that aligns with the CDC’s 2022 guidelines without alienating the people you serve.
Decoding the ‘unexpected’ result
The term “failed drug test” is loaded with negative connotations that can damage patient trust. A more accurate and productive term is an “unexpected” or “inconsistent” result. This reframes the outcome not as a failure, but as a clinical signal that requires further investigation. An unexpected result can mean several things:
- The prescribed drug is absent.
- An illicit or non-prescribed drug is present.
- A metabolite is present without the parent drug.
- A parent drug is present without its expected metabolites.
These results don’t automatically point to misuse. They can be caused by metabolic variations, drug-to-drug interactions, or even cross-reactivity from common over-the-counter medications. Treating an unexpected result as the start of a conversation, not the end of one, is the foundation of effective stewardship.
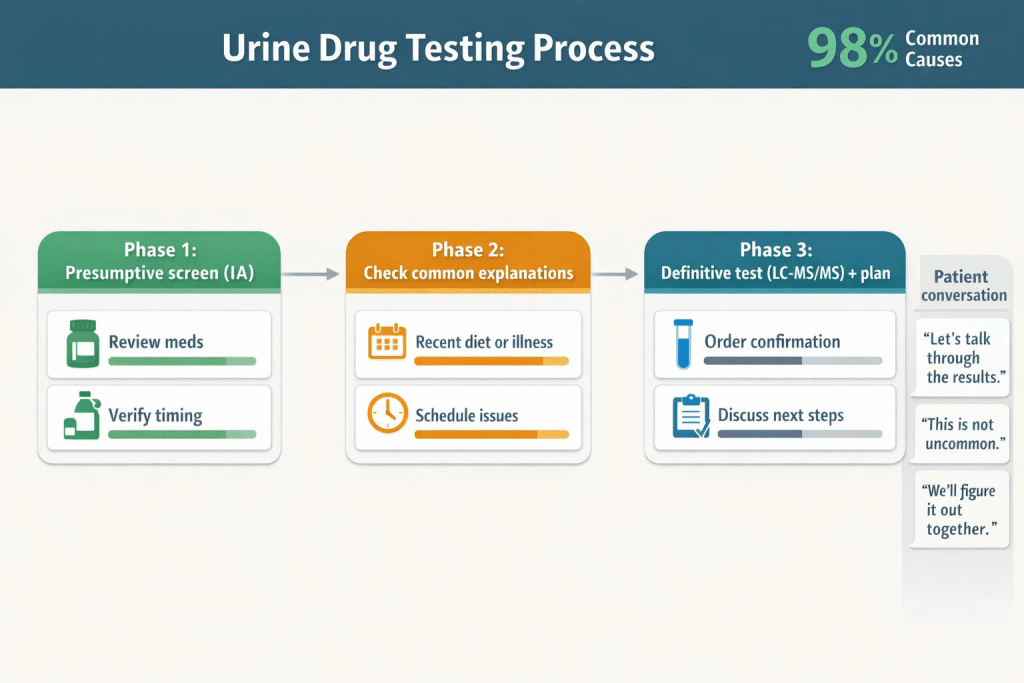
A calm, step-by-step interpretation path helps patients and clinics treat unexpected results as a signal to investigate—before assuming non-adherence or diversion.
Understanding cross-reactivity and false positives
One of the most common reasons for a confusing result is cross-reactivity, where a substance has a similar chemical structure to the target drug, triggering a positive on an initial screen. This is a known limitation of immunoassay (IA) screening tests, the technology used in most point-of-care cups and dip cards.
While these screens are an essential first step for their speed and affordability, it’s vital to understand their limitations. For example, research from Mayo Clinic Labs confirms that common OTC medications are frequent culprits for false positives.
Common Substances with High Cross-Reactivity Potential
| Substance | Can Cause False Positive For |
|---|---|
| Dextromethorphan (Cough Syrup) | Opioids, PCP |
| Diphenhydramine (Benadryl) | Methadone, Opioids |
| Quetiapine (Seroquel) | Methadone, TCAs |
| Quinolone Antibiotics (e.g., Levaquin) | Opioids |
| Ibuprofen / Naproxen (NSAIDs) | Barbiturates, Cannabinoids |
Having this knowledge on hand allows you to immediately cross-reference a patient’s medication list against an unexpected result, reducing unnecessary anxiety and building confidence in your clinical process.
The critical difference: presumptive vs. definitive testing
A modern drug testing protocol is a two-step process. Understanding the role of each step is key to making it both cost-effective and clinically sound.
Step 1: Presumptive screening (The ‘what’)
Presumptive tests, like the reliable 12-panel drug test cups, are designed to be a rapid, sensitive, and affordable first line of inquiry. These are immunoassay tests that provide a simple positive or negative result for multiple drug classes.
- Purpose: To quickly and cost-effectively rule out the presence of many common substances.
- Strength: Excellent for verifying adherence when results are as expected. They are fast, easy to administer, and allow for immediate clinical conversations.
- Limitation: They are prone to cross-reactivity and may produce false positives. Critically, standard immunoassays often miss synthetic opioids like Fentanyl or Buprenorphine, which could lead to a “false negative” that is misinterpreted as adherence when a dangerous substance is actually present.
Step 2: Definitive confirmation (The ‘which’ and ‘how much’)
When a presumptive screen yields an unexpected result, a definitive test is the essential next step. These tests, typically using Liquid Chromatography with Tandem Mass Spectrometry (LC-MS/MS), are performed in a laboratory.
- Purpose: To confirm the specific drug and its metabolites present in the sample, eliminating any ambiguity from the initial screen.
- Strength: Highly specific and sensitive. An LC-MS/MS test can distinguish between codeine and morphine, identify specific synthetic compounds missed by IA screens, and quantify the amount of substance present. It is the gold standard for accuracy.
- Role: Definitive testing is the patient’s best advocate in a dispute. It provides the scientific proof needed to resolve a potential false positive or clarify a complex metabolic profile.

Screening tests are fast but imperfect; confirmation testing adds specificity and protects both patient safety and opioid stewardship decisions.
The science of interpretation: metabolic mapping
Sometimes, an unexpected result isn’t a false positive but a true metabolic fact. Many opioids metabolize into other opioids, which will then appear on a drug test. A patient taking their medication exactly as prescribed can have a test show a substance they technically never ingested.
Understanding these pathways is critical to avoid incorrect accusations of misuse. For example:
- Codeine metabolizes into Morphine.
- Oxycodone partially metabolizes into Oxymorphone.
- Hydrocodone metabolizes into Hydromorphone.
If a patient is prescribed Codeine, their test should show both Codeine and Morphine. Seeing only Morphine could suggest the patient is taking unprescribed Morphine instead. Conversely, seeing both proves adherence. This level of metabolic mapping helps differentiate compliance from diversion and validates a patient’s legitimate use.

Metabolites can appear even when patients take medication exactly as prescribed—mapping the pathways prevents misinterpretation and supports fair clinical decisions.
A provider’s toolkit for building trust
An effective drug testing program is built on a framework of clear policies, consistent application, and open communication. This reduces patient anxiety and protects your clinic from regulatory scrutiny.
The anatomy of a pain management agreement
A pain management agreement, or “pain contract,” should be a tool for education, not just enforcement. It sets clear expectations for both the patient and the provider. A strong agreement should outline:
- The clinic’s medication and refill policies.
- The frequency and nature of drug testing (e.g., random, scheduled).
- The specific actions that will be taken in response to unexpected results, emphasizing a non-punitive, investigatory approach first.
- Patient responsibilities, such as disclosing all medications from all providers.
This document becomes the reference point for all conversations, ensuring fairness and transparency.
Implementing a clear testing protocol
In line with CDC guidelines, your protocol should define when and why you test. A standardized approach ensures all patients are treated equitably and provides a defensible framework during an audit. This protocol should specify the conditions that trigger a definitive confirmation test, such as any result inconsistent with the patient’s prescriptions. Documenting the medical necessity for every confirmation test is crucial for both compliance and payer reimbursement.

A clear UDT protocol improves compliance and reduces patient friction—standardizing when to confirm and how to document supports safer prescribing and audit readiness.
Partnering for patient safety and compliance
Integrating a robust drug testing protocol is no longer optional for pain management clinics. It is a core component of patient safety, risk management, and responsible opioid stewardship. By combining fast, reliable presumptive screening with a clear, evidence-based process for definitive confirmation, you create a system that protects your patients and your practice.
The first step is ensuring your team has access to accurate and affordable screening tools. At 12 Panel Now, we provide CLIA-waived and FDA-approved testing supplies that deliver the reliability you need to make confident clinical decisions right from the start.
Explore our full range of CLIA-waived testing supplies to build the foundation of a drug testing protocol that fosters trust and ensures adherence.