Oral Fluid Drug Detection Windows: The 2026 Guide to Timeframes and Testing Accuracy

If you are evaluating your organization’s drug testing protocol in 2026, you have likely noticed a monumental shift in the industry. Over the past two years, employer adoption of oral fluid screening has surged by 74%.
While traditional urine analysis remains the historical gold standard for long-term compliance, oral fluid (saliva) has quickly become the definitive tool for Drug Detection of recent use and active impairment. With the saliva-based technology market projected to reach $3.5 billion by 2030, understanding the exact detection windows and scientific mechanics of oral swabs is no longer optional for decision-makers—it is critical.
Whether you are an employer upgrading to the latest DOT and SAMHSA guidelines, or a clinic comparing testing methodologies, you need clear, data-backed insights. Let’s break down how oral fluid detection actually works, why it differs from urine testing, and the specific timeframes you can expect for common substances.
The Recency Advantage: Why Saliva Testing Targets the “Now”
The fundamental difference between oral fluid and urine testing comes down to a single concept: timelines. Urine testing is excellent at identifying past behavior, but it often falls short when you need to know if someone is under the influence right now.
Saliva tests can detect substances like THC within minutes of ingestion. In contrast, urine tests can take anywhere from 3 to 6 hours for the body to process a substance into the detectable waste products (metabolites) required for a positive result.
Beyond speed, 58% of employees prefer saliva testing because it respects privacy and is highly efficient. For employers, the value lies in observed collection. Because an oral swab is administered directly in front of the evaluator, it is virtually impossible to cheat, completely eliminating the costly adulteration risks associated with unobserved urine collection.
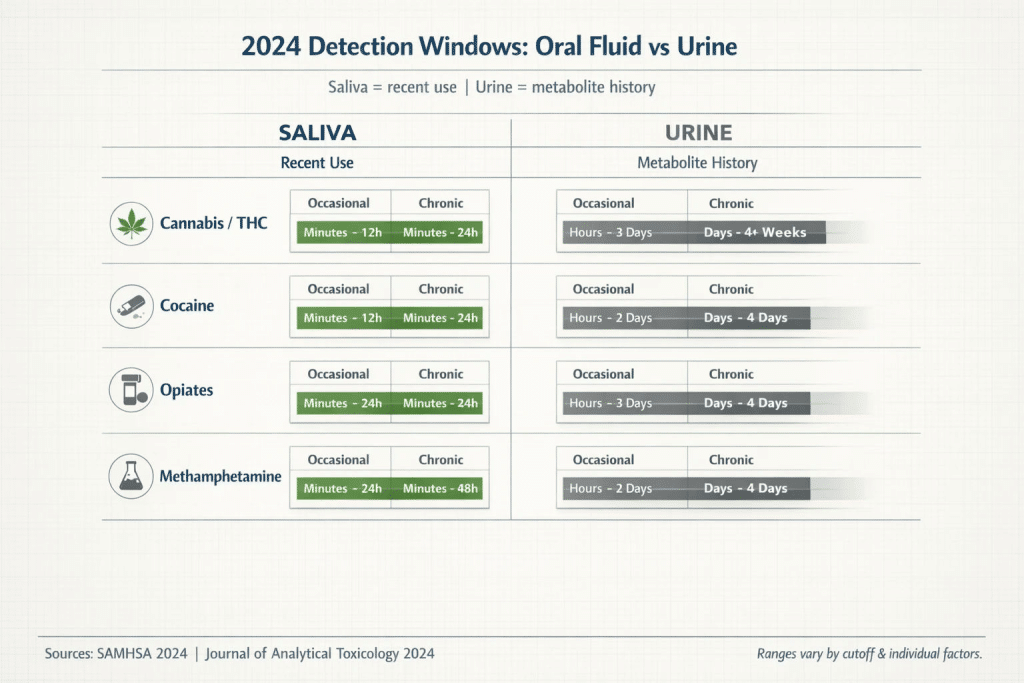
Side-by-side windows clarify what each test is built to detect: oral fluid trends toward recent use, while urine captures longer metabolite history. Use ranges as planning guidance, not guarantees.
2026 Saliva Drug Detection Timeframes
Detection windows are not universal. They fluctuate based on the specific drug, the user’s frequency of consumption, and the cut-off levels of the test itself. Below is a detailed breakdown of oral fluid detection windows for the most commonly screened substances.
Cannabis (THC)
Cannabis is the most searched and scrutinized substance in drug testing. Because THC is highly fat-soluble, it behaves differently than water-soluble drugs.
- Occasional Use: Detectable within minutes, typically lasting 12 to 24 hours.
- Chronic/Heavy Use: Can occasionally linger up to 30 hours in saliva.
- Note: Unlike urine, where THC metabolites can linger for 30+ days in heavy users, saliva clears THC rapidly. This makes it an incredibly fair test for legal-state employers who want to screen for on-the-job impairment rather than weekend recreational use.
Cocaine
- Detection Window: Minutes up to 24 to 48 hours.
- Cocaine metabolizes quickly in the bloodstream. Saliva captures the immediate presence of the drug, making it highly effective for post-accident screening.
Opiates (Heroin, Morphine, Codeine)
- Detection Window: Minutes up to 24 to 36 hours.
- Oral fluid testing is highly sensitive to opiates, correlating closely with peak intoxication levels in the user’s bloodstream.
Methamphetamine & Amphetamines
- Detection Window: Minutes up to 48 hours.
- Because amphetamines stimulate the central nervous system rapidly, they appear in oral fluid almost simultaneously with their effects on the body.
The Parent Drug Secret: Why Saliva and Urine Results Sometimes Mismatch
One of the most common questions decision-makers face is: “Why did a subject fail an oral fluid test but pass a urine test on the same day?” (Or vice versa).
The answer lies in pharmacokinetics—specifically, the difference between parent drugs and metabolites.
When a person consumes a drug, the original, unprocessed substance (the parent drug) immediately enters the bloodstream. Because your salivary glands filter blood plasma to create saliva, that parent drug transfers directly into your mouth via a process called passive diffusion. Therefore, an oral swab detects the parent drug, signaling active intoxication.
Urine tests, however, are looking for metabolites. These are the chemical byproducts created after the liver has processed the parent drug. This processing takes hours. If you test someone immediately after they consume a substance, their urine will likely be clean (because the body hasn’t created the metabolites yet), but their saliva will trigger a positive result.

When a test targets parent drug vs metabolites, the detection window shifts. This visual shows why oral fluid aligns with recent use while urine can stay positive longer.
Factors That “Break” the Detection Window
While average timeframes are helpful, oral fluid detection is influenced by complex physiological variables. Understanding these factors helps administrators interpret borderline or unexpected results with confidence.
1. The pH Factor and Ion-Trapping
This is a critical variable many providers fail to explain. The acidity (pH level) of a person’s saliva directly impacts drug concentration. When saliva is highly acidic, basic drugs (like methamphetamines and cocaine) become trapped in the oral fluid—a phenomenon known as “ion-trapping.” This can actually increase the concentration of the drug in the saliva, extending the detection window slightly. Conversely, acidic drinks or candies might temporarily alter the pH, but the saliva regenerates so quickly that the baseline returns within minutes.
2. Salivary Flow Rate and Hydration
How much saliva a person produces matters. Stimulating saliva production (by chewing food or drinking water) dilutes the concentration of the drug temporarily. However, because the parent drug is constantly diffusing from the blood into the saliva, this dilution is fleeting.
3. Xerostomia (Dry Mouth)
Many illicit substances, as well as severe dehydration, cause dry mouth. If a subject suffers from xerostomia, it can make collecting an adequate sample difficult. Fortunately, modern, high-quality FDA-approved oral swabs are designed with advanced saturation indicators that ensure a sufficient sample is gathered even in low-flow situations.
Cheating the Uncheatable
Can users “beat” an oral swab using mouthwash, vigorous brushing, or chewing gum? The science says no. While a harsh mouthwash might strip the outer layer of oral tissue temporarily, fresh saliva begins pooling back into the mouth immediately, carrying the parent drug with it from the bloodstream. This makes oral swabs highly resilient against tampering.

Detection windows aren’t fixed. pH, flow rate, hydration, and lab cutoffs can widen or narrow what oral fluid detects—helpful for interpreting borderline or unexpected results.
The Employer Comparison Hub: Transitioning Your Testing Strategy
With the Department of Transportation (DOT) integrating oral fluid testing into their 49 CFR Part 40 final rule, and SAMHSA continuously refining oral fluid guidelines, legal defensibility is higher than ever.
If you are structuring a testing program in 2026, you need a balanced approach. Here is how oral fluid compares to other methods:
- Oral Fluid: Best for reasonable suspicion, post-accident, and random testing. It offers high precision for recent use, 99% reliability with CLIA-waived products, eliminates privacy concerns, and completely mitigates adulteration risks.
- Urine Analysis: Best for comprehensive pre-employment screening where identifying a historical pattern of use is more important than identifying active impairment.
- Hair Follicle Testing: Best for strict zero-tolerance environments evaluating long-term historical use (up to 90 days), though it comes with a high cost and longer turnaround times.
By aligning the right test with the right scenario, organizations save capital, respect employee privacy, and drastically reduce their legal risk profile.

For workplace programs, the best test is the one that matches your risk profile and compliance needs. This scorecard compares practical tradeoffs and highlights where oral fluid excels for recent-use screening.
Next Steps for Your Testing Program
Implementing a robust, defensible drug testing protocol requires balancing accuracy, cost-efficiency, and ease of use. Oral fluid testing delivers on all three fronts—provided you equip your team with supplies that meet rigorous industry standards.
When evaluating vendors for your testing supplies, ensure you are prioritizing suppliers that offer CLIA-waived, FDA-approved products with demonstrated 99% reliability. By standardizing your inventory with high-quality oral swabs and multi-panel test cups, you empower your organization to make confident, compliant safety decisions every single day.
Frequently Asked Questions
Can passive exposure to marijuana smoke trigger a positive saliva test?
It is highly unlikely. While initial exposure might leave trace amounts of THC in the oral cavity, it dissipates rapidly. High-quality oral swabs have specific cut-off levels designed to differentiate between active consumption and incidental passive exposure.
Are saliva tests FDA-approved and legally defensible?
Yes. Providing you source from a reputable supplier, modern oral fluid test kits are FDA-approved, CLIA-waived, and offer a 99% accuracy rate. Since the DOT and SAMHSA guidelines were updated, oral fluid is a federally recognized and legally defensible testing medium.
How quickly can a drug be detected in saliva after use?
In many cases, almost immediately. Unlike urine, which requires metabolic processing, saliva pulls parent drugs from the bloodstream within minutes of ingestion.
Is oral fluid testing more affordable than urine testing?
When evaluating total program cost, yes. While the baseline unit cost of a premium multi-panel cup versus an oral swab might be comparable, saliva tests eliminate the need for specialized bathrooms, same-sex collection observers, and the costs associated with “shy bladder” delays














