Interpreting Oral Swab Drug Test Results & Cut-off Levels

Staring at a rapid drug test device waiting for a result is an inherently stressful experience. Whether you are an employer ensuring safety compliance, or an individual undergoing a screening, that small plastic window holds a lot of weight.
But as we navigate through 2026, reading an oral fluid test involves much more than simply looking for lines. The recent 2025 Department of Transportation (DOT) and SAMHSA regulatory updates have completely transformed the saliva testing landscape, introducing new, highly specific cut-off levels that change how we interpret results—especially for THC.
If you are trying to understand a faint line, decipher what an “invalid” test means, or prepare for a medical review due to a suspected false positive, you need accurate, up-to-date information. Let’s decode exactly what your oral swab drug test results are telling you.
Reading the Lines: What Positive, Negative, and Invalid Really Mean
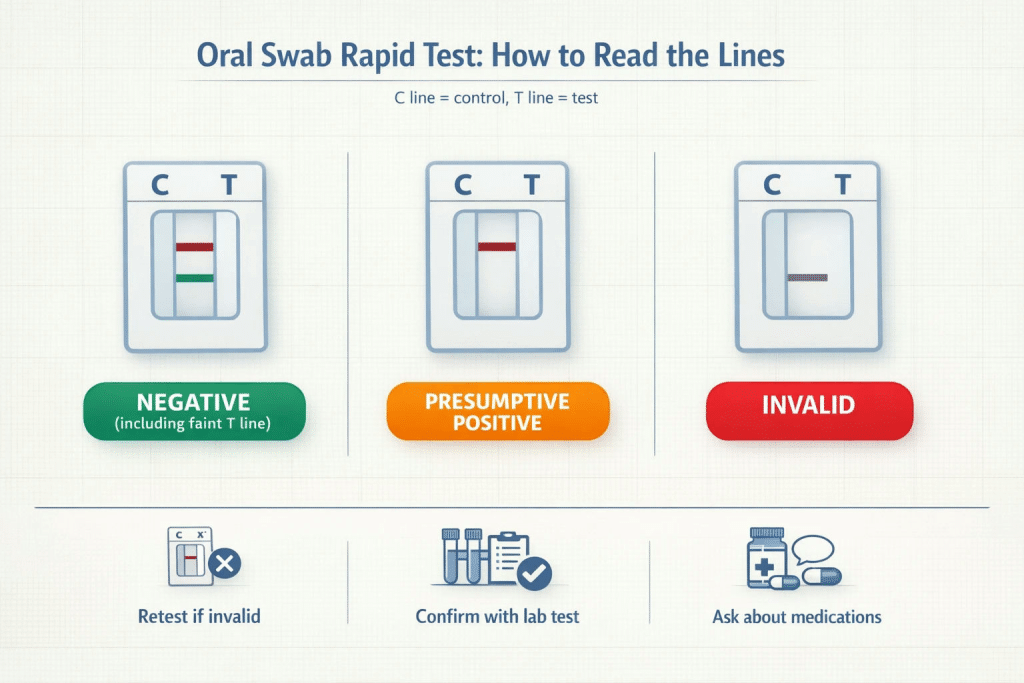
The most common anxiety surrounding rapid oral drug tests is the “faint line.” To interpret a test accurately, you have to understand the binary nature of the Control (C) and Test (T) regions.
- Negative (Pass): You will see a line in the Control (C) region and a line in the Test (T) region. Crucially, the intensity of the T-line does not matter. A faint line, a barely-there shadow, or a bold red streak all mean the exact same thing: the substance was not detected above the cut-off level. It does not mean you “barely passed” or have trace amounts in your system.
- Presumptive Positive (Fail): You will see a solid line in the Control (C) region, but no line in the Test (T) region. The lack of a line indicates that the specific drug has bonded to the reagents, preventing the color indicator from showing up.
- Invalid: If there is no line in the Control (C) region, the test is invalid, regardless of what happens in the Test region. This usually means there was insufficient saliva collected or the device malfunctioned. The test must be discarded, and a new swab administered immediately.
The “Parent Drug” Advantage: Why Saliva is the Truth Teller
One of the reasons oral fluid testing has become the gold standard for post-accident and reasonable-suspicion testing is its diagnostic precision.
Urine tests detect metabolites—the inactive byproducts left over days or weeks after a body processes a drug (like THC-COOH). Saliva, however, detects the parent drug—the active, unmetabolized substance (like Delta-9-THC) present in the blood and oral mucosa. This means an oral swab specifically indicates recent use, effectively answering the question, “Is this person under the influence right now?” rather than, “Did this person use a substance last weekend?”
Understanding Cut-Off Levels in the 2026 Landscape
A “cut-off level” is the exact concentration of a substance (measured in nanograms per milliliter, or ng/mL) that must be present to trigger a positive result. If an individual has 3 ng/mL of a substance in their saliva, and the cut-off is 4 ng/mL, the test will read as negative.

The 2025 DOT and SAMHSA updates completely rewrote the rules for cut-off levels, primarily to adapt to a world where legal CBD use is ubiquitous.
Under current federal standards, the initial screening cut-off for THC in oral fluid is heavily restricted to 4 ng/mL, specifically targeting Delta-9-THC. If the initial rapid Enzyme Immunoassay (EIA) test flags positive, it goes to the lab for a Gas Chromatography/Mass Spectrometry (GC/MS) confirmation test, which has an even stricter cut-off of 2 ng/mL.
This Delta-9 specificity is a massive win for reliability. It virtually eliminates the risk of a broad-spectrum CBD product triggering a false positive, ensuring that rapid oral tests evaluate true impairment accurately.
What Happens After a Positive Saliva Drug Test Result?
When an on-site rapid oral swab lacks a T-line, it is officially classified as a “Presumptive Positive.” It is critical to understand that a rapid test result is not legally or medically final until confirmed by a laboratory.

Once a lab confirms the positive result via GC/MS testing, the results are sent to a Medical Review Officer (MRO). The MRO is an independent, licensed physician tasked with determining if there is a legitimate medical explanation for the positive result.
Factors Leading to False Positives (The MRO Defense Kit)
While lab-confirmed oral fluid tests boast a 97% accuracy rate, the initial rapid EIA screenings are susceptible to cross-reactivity. This happens when the chemical structure of a legal medication mimics an illicit drug closely enough to fool the initial screen.
If you are contacted by an MRO, you should have your prescription bottles and over-the-counter (OTC) medication list ready. Common culprits for cross-reactivity in oral testing include:
- Bupropion (Wellbutrin): Frequently triggers a false positive for amphetamines.
- Vicks Inhalers (L-methamphetamine): Can occasionally trigger an initial presumptive positive for methamphetamines, though a lab confirmation will easily distinguish it from illicit D-methamphetamine.
- Dextromethorphan (Robitussin): Can sometimes trigger false positives for PCP or opiates on an initial rapid screen.
- Poppy Seeds: While much less likely to trigger a saliva test than a urine test, massive consumption can theoretically cross-react with opiate screens.
The MRO will verify your prescriptions. If your prescribed medication caused the flag, the MRO will overturn the result and report it to the employer as a “Negative.”
Detection Windows: When Timing Matters
When evaluating drug testing methods, understanding the detection window—the period during which a test can accurately detect a substance—is essential.

Oral fluid testing is explicitly designed to catch recent use.
- Immediate Detection: Saliva tests can detect drug usage as recently as 30 minutes ago. By contrast, urine tests often require 2 to 6 hours for a substance to metabolize and show up.
- Shorter Window: The detection window for saliva closes rapidly, typically within 24 to 48 hours for most substances. Urine testing can detect metabolites for 3 to 30 days, while hair follicle testing can look back up to 90 days.
This tight 48-hour window makes oral fluid the most defensible method for determining immediate workplace or roadside safety.
Next Steps for Reliable Testing
Understanding the nuance between a presumptive positive, a faint line, and the intricacies of 2026 cut-off levels is what separates an anxious testing process from a confident one. Whether you are scaling a corporate drug-free workplace program or managing a clinical facility, the integrity of your results starts with the quality of your supplies.
Choosing FDA-approved, CLIA-waived testing devices guarantees you are working with tools that adhere strictly to modern compliance standards. By utilizing reliable, highly accurate multi-panel oral swabs, you ensure that every test administered is defensible, clear, and fair to all parties involved.
Frequently Asked Questions (FAQ)
Are rapid oral swab tests reliable?
Yes. High-quality, FDA-approved, and CLIA-waived rapid tests are incredibly reliable for initial screenings. When paired with lab-based GC/MS confirmation, oral fluid testing maintains a clinically reviewed accuracy rate of over 97%.
I have a faint line on my T-region. Do I need to re-test?
No. A faint line is a negative result. Re-testing is only necessary if the Control (C) line fails to appear, which indicates an invalid test.
Will second-hand marijuana smoke cause a positive saliva test?
Due to the strict 4 ng/mL cut-off levels updated by the DOT in 2025, passive exposure to second-hand smoke is highly unlikely to trigger a presumptive positive on an oral fluid test.
Can I wash my mouth out to beat a saliva test?
Because saliva is constantly regenerating from the blood plasma through the oral mucosa, mouthwashes, mints, and chewing gum cannot “flush” the parent drugs out of your system. They may dilute the sample momentarily, but high-quality oral swabs contain sponge indicators that require adequate, undiluted fluid saturation to display a Control line.